Ignored Warnings Left the Military Health System Unprepared

Navy Hospital Corpsman 3rd Class Kimberly Wyss, from Ventura, California, dons surgical gloves aboard the hospital ship USNS Mercy, March 29, 2020. (Photo: U.S. Navy / Mass Communication Specialist 2nd Class Ryan M. Breeden)
New Yorkers crowded into Manhattan’s West Side in defiance of social distancing bans to welcome the USNS Comfort’s glide into the city’s harbor on March 30. In addition to providing some relief to the city’s besieged hospitals, the large white ship with its red crosses gave the appearance of a powerful symbol of the military’s ability to respond to a crisis. What most of the apparently grateful people lining the waterfront did not know is that the military’s health system has been gutted in recent years despite repeated warnings from medical professionals.
The public show of military doctors aiding in the coronavirus response belies the fact that the military health system lacks the ability to handle even the routine health needs of the services during normal conditions.
The public show of military doctors aiding in the coronavirus response belies the fact that the military health system lacks the ability to handle even the routine health needs of the services during normal conditions. A Defense Department Inspector General investigation found, for example, that because of a shortage of doctors, the Langley Air Force hospital in Virginia had only one provider for every 1,600 patients even though regulations require there be only 1,250 patients per provider—a regulation that still leaves a burdensome caseload. These shortages, the inspector general found, meant patients “may have been at risk of increased health complications due to longer wait times.”
As will be discussed below, those shortages are due in large part to placing a much higher priority on spending for pet weapons programs. Evidence of this can be seen in the service’s most recent so-called unfunded priorities list, through which services try to get money for programs that were not included in the department’s regular annual budget request. The Navy did request $11.6 million to upgrade the USNS Mercy hospital ship, but that was the only health care related request on any of the service’s wish lists. They devoted the rest of their $5.42 billion request to things like a submarine, F-35s, and missiles. The Army is requesting over $7 billion, more than half of which is meant to pay for current overseas operations. Of what remains, the Army has earmarked a third to purchase helicopters, armored vehicles, and simulators. The rest is to build barracks and childcare centers, and to pay for building renovations. None goes to health care. The Air Force similarly did not request additional funds for health care. Unless quick action is taken, the services may not have enough doctors and nurses to respond to either a domestic crisis or battlefield needs when the nation goes to war.
The nation has already seen a preview of the coming crisis in military medicine when the Army had to reach out to retired military doctors and medics to return to service as part of a voluntary recall to help fight the coronavirus. Fortunately, many were listening because within days of notifications being sent to more than 800,000 former soldiers, approximately 25,000 volunteers stepped forward to backfill positions in military treatment facilities as troops deployed to the field hospitals now popping up in American cities to deal with patients stricken by the virus.
Undoubtedly, military leaders resorted to such measures due to the scale of the coronavirus response. But a review of government reports and medical journal articles, as well as conversations with military doctors, shows that years of reduced spending on the Defense Department’s health services, reductions to the medical corps staff, and efforts to outsource military health care to civilian hospitals strained the system long before the virus emerged and set the stage to have to resort to volunteers.
Ignored Warnings
The Government Accountability Office warned in February 2018 that the military health system lacked the capacity to handle routine medical needs, to say nothing of a surge like the one we are experiencing with the coronavirus or that would result the next time we go to war. Service leaders interviewed for the study reported shortages of doctors with key specialties including general surgery, orthopedic surgery, and family medicine. “Until DOD is able to alleviate gaps in critical specialties, it may be hindered in its ability to provide medical support for its servicemembers during wartime,” the report said.
Yet from its peak in 2011 to the present, the budget for military health care largely remained flat. Spending levels have not even been keeping up with inflation, which amounts to a spending cut. In an effort to make the accounts balance, the Defense Department proposed eliminating 15,000 military doctors and nurses in the fiscal year 2018 budget request. Pentagon leaders want to outsource a large part of military medical care to civilian hospitals to allow its physicians to focus on battlefield medicine and free up manpower slots for other combat-related jobs. The leaders of the congressional armed services committees received a letter on July 19, 2019, urging them to reject the plan. The letter, signed by 17 medical associations including the American Academy of Family Physicians, the American Medical Association, and the Society of Critical Care Medicine, warned that the military health system was already overburdened and struggling to “handle the basic health needs of our country’s Armed Forces and their families.” Congress listened this time and told the Pentagon to carefully review the medical needs of the services further before making any new cuts, but earlier changes had already left the military health service in a precarious position.
In the last few years before the coronavirus began spreading around the globe, military doctors flooded medical journals and the nation’s op-ed pages with warnings of an impending crisis within the military’s medical corps. A smaller medical corps increases the burdens placed on the remaining personnel, a burden that is having a cascading effect throughout the entire system. A group of six Army and Air Force doctors published an article in April 2019 detailing faculty burnout at the military’s graduate medical education programs because of an increasing number of deployments and a lack of administrative support. The authors warned of the impact on the medical corps in the future. “Physician burnout presents a direct and immediate threat to the vitality of a [graduate medical education] program and may adversely affect the quality of education delivered.”
In June 2019 retired Vice Admiral Michael Cowan, the Navy’s 34th surgeon general, warned that the military’s medical services had already been stripped of their excess capacity and any further cuts could permanently damage the entire system. “My college physics professor was fond of stating that a 20 percent change in a physical system was a threat to the system itself,” he wrote. “The current proposal to implement a 20 percent reduction in forces without compensating resources represent an existential threat to military medicine.”
Three former Army, Navy, and Air Force surgeons general published a column in July 2019 prophetically warning that the medical corps operated near maximum capacity under normal circumstances and had little ability to respond to a crisis such as a surge in medical needs when a war breaks out. “If even one of these ‘high-risk, high-regret’ consequences unfolds, the percent of those dying from wounds will increase, the all-volunteer force will suffer, and we may be forced to again draft medical personnel—including physicians,” they wrote.
Military Health Spending Flattened as Procurement Costs Increased
Looking at historical budget data provides some insight into defense priorities. Pentagon funding ebbs and flows over time based on the state of the world and domestic politics. This has been especially true over the last 20 years. While the topline defense budget has trended up during that time, spending levels for the military health system stagnated and, because of inflation, have been effectively cut. The White House proposed a 5% increase for the overall Pentagon budget for 2020, but spending on the military health system went down by 2.3% from 2019 to 2020.
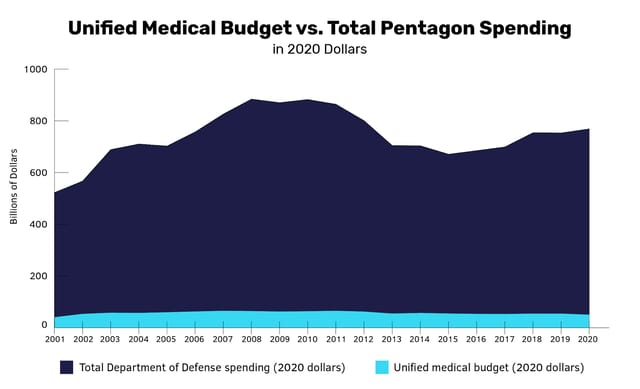
Data shows the divergence between overall Pentagon spending and the Unified Medical Budget (UMB) in 2020 US dollars. At the height of the total Pentagon budget, spending was highest between 2008 and 2010, averaging $815.1 billion in 2020 dollars. Total Pentagon and UMB spending was calculated using official DoD and selected economy-wide deflator indices from the Office of the Under Secretary of Defense (Comptroller). (Chart: POGO; data sourced from the Office of the Under Secretary of Defense (Comptroller).)
The Budget Control Act of 2011 that, in part, imposed caps on discretionary spending included caps on spending on defense. Pentagon leaders and their allies found some ways around the caps, most often by sneaking regular military spending into the Overseas Contingency Operations fund. Still, the Budget Control Act did force service leaders to make some choices.
As is often the case, though, they placed top priority on acquisitions projects at the expense of essential missions like maintenance and medical capabilities. In 2016, the Pentagon spent $177.5 billion on major weapon systems. That spending increased to $243.4 billion in the 2021 budget request, a 37% increase to pay for things like five littoral combat ships, a class of ships that have never worked properly and the Navy wants to scrap; and $2.85 billion for the Air Force’s KC-46 aerial refueler program, an aircraft so full of problems that airmen aren’t allowed to use them in training. While lawmakers lavished money on the procurement portion of the budget, spending levels on the military health system remained stagnant. Only after a worldwide health crisis made clear how desperate the shortages were in the military medical community did anyone seek to do something about it. The coronavirus stimulus package included $3.8 billion for the military to purchase personal protective equipment, increase the capacity of its hospitals, and fund research into a vaccine.
Outsourcing Military Health Care Reduces Capacity
During the 2020 budget cycle, Pentagon leaders wanted to cut more than 17,000 uniformed doctors, dentists, nurses, and medical support staff from the three service medical corps. Citing cost concerns and a medical staff filled with specialties not needed on the battlefield, the proposal would have seen the Army’s medical staff shed 7,300 positions while the Navy and Air Force would have each cut approximately 5,300. The proposal found some support on Capitol Hill, but was ultimately rejected in the final version of the national defense authorization act pending further study on the potential impacts.
The proposed cuts did come from earlier studies about the military health system. A 2017 study by the Institute for Defense Analyses found that the costs associated with operating military hospitals did not correspond with military medicine’s primary mission of treating the troops wounded in combat. The researchers found that the stateside military hospital staff dealt mainly with family health issues like newborn care, pregnancies, substance abuse, and metabolic disorders. Their deployed counterparts faced very different medical challenges. They treated open wounds to the head, neck, and trunk, fractured limbs, crushing injuries, and tissue infections. The concern was that the routine treatment of patients in military hospitals in the United States was not providing military medical professionals the kind of experience necessary to prepare them to treat combat-wounded troops. According to the report’s author, “the lack of appropriate case mix in MTFs [military treatment facilities] affects the ability of medical personnel to respond most effectively to in-theater trauma events.” But military health professionals trained in the current system perform heroic service on the battlefield, and as will be discussed in more detail below, have produced remarkable results.
Increasing the number of troops by cutting medical staff means that the remaining medical professionals would be even more overburdened.
Outsourcing family and veteran care to civilian hospitals and cutting uniformed medical staff would, according to the proposals, allow the remaining uniformed medical staff to focus their efforts on battlefield trauma care. To that end, military trauma specialists would continue to spend time in civilian hospital emergency rooms in cities around the country where they gain experience treating victims of accidents and violence. By eliminating these uniformed medical positions, so the thinking goes, the services would be able to increase the number of personnel in combat roles while staying within the existing end strength caps. However, this course of action would actually make the problem worse. Increasing the number of troops by cutting medical staff means that the remaining medical professionals would be even more overburdened.
The Pentagon has already taken steps to shift the burden of military medical care to the civilian sector. The Defense Department downgraded military hospitals in Fort Knox, Kentucky, Fort Jackson, South Carolina, and Fort Sill, Oklahoma, to outpatient clinics in the last five years. In 2016, Fort Knox’s Ireland Community Hospital closed its emergency room, stopped performing major surgeries, and stopped delivering babies. People requiring that kind of care were instead sent to community hospitals in the surrounding communities. In the case of Fort Knox, the civilian medical system did not have the necessary capacity to handle the sudden influx of patients. A local bank ended up donating $1.5 million to fund the expansion of a clinic to treat military families and retirees. Military families nation-wide report difficulty in finding health care providers in the Defense Department’s TRICARE civilian health care plan.
On the business side of things, outsourcing makes a great deal of sense to the civilian hospital administrators. The Pentagon provides them with a lot of business and pays its bills on time. As with all things related to the military, contracts for the military’s TRICARE civilian health care plan are lucrative. The Pentagon awarded California-based Health Net Federal Services a $17.7 billion contract in 2016 to manage the military’s western TRICARE region for five years. At the same time, Kentucky-based Humana received a $40.5 billion contract to manage the eastern region for five years. The Pentagon can and does use contractor medical personnel for deployments, but contractors are expensive. One job posting on the Defense Health Agency’s website for an emergency room physician position in South Korea pays as much as $365,000 per year. When a contracting firm’s billing rates are added on top of the salary, the cost to the taxpayer could more than double. A previous POGO investigation found the annual billing rate for contract nurses was, on average, 65% more than the federal employee’s average salary.
One military doctor acknowledged that military doctors spend most of their time treating non-combat related issues. “This is our biggest mission,” said Army Lieutenant Colonel Robert Mabry, an emergency medical doctor, during a February 2016 hearing before the House Armed Services Committee. He continued, though, that “it is our wartime mission that makes us unique and justifies our cost to the Nation.” Because as competent as the civilian medical health care professionals may be, they do come with a significant drawback: They do not deploy with the troops when the troops go to war. This is a point that has been acknowledged on Capitol Hill. “It takes guys and girls in uniform to get our soldiers to the right level of care in that magic hour. And if they’re not there, we have soldiers, sailors, airmen and Marines that die,” said Representative Trent Kelly (R-MS) in a December 2019 hearing. In addition, because the military can’t force people to take contractor positions, many of the doctors who will volunteer for the most dangerous contractor postings will be those who can’t find a job anywhere else. “I’ve seen less qualified physicians volunteer for these challenging roles, or the uniformed providers will be sent,” Dr. Bob Adams, a retired Army doctor writing in a July 2019 column for USA Today, said. “This can hurt quality of care and military retention, as well as potentially greatly increasing the cost.”
The Military Health System’s Contributions to Saving Lives
The Military Health System comprises all of the uniformed, civilian, and contract personnel for the Army, Navy, and Air Force. The system operates 51 military hospitals and 424 smaller clinics on bases all around the world where service members, military dependents, and veterans receive care.
But the Military Health System’s mission goes far beyond just providing care; it also educates future military medical professionals. The Uniformed Services University has served as the West Point of the medical branches for all of the services since its creation in 1972. That said, the university has faced criticism over the years for the high cost of educating doctors when compared to civilian medical schools. Each student at the university costs taxpayers more than $133,000 per year when even the most expensive private medical school costs $68,000 a year. The services also recruit doctors through the Health Professions Scholarship Program where medical students attending civilian schools agree to serve a minimum period on active duty in return for tuition and a monthly stipend. The Defense Department uses retention bonuses of up to $59,000 a year to preserve this capacity. It’s unclear whether this investment pays off or not. The Government Accountability Office reported in 2019 that “DOD does not consistently collect information on retention of physicians and dentists” who receive those bonuses.
While it is expensive to educate doctors through the military, those doctors not only fill an important role while they serve in uniform but also make up a significant portion of the total population of doctors in the United States. Without the military, the United States would experience even more of a shortage in the number of doctors than we already do. In 2019, more than 1,200 students begin medical school at either the Uniformed Services University or at a civilian medical school with a military scholarship. Future military doctors made up approximately 5% of the country’s 21,869 new medical students in the 2019-2020 academic year.
The pipeline of military doctors will become increasingly important as demand for doctors grows during the next decade: According to a study by the Association of American Medical Colleges, the shortfall of American doctors could be as high as 121,900 by the year 2032.
The military health system also makes significant contributions to the overall body of medical knowledge. Advances in trauma medicine by military doctors, nurses, and medics have been nothing short of phenomenal. As a result of those military medical advances, 70% of service members wounded in action during WWII survived, 76% of those wounded during Vietnam survived, and, incredibly, more than 90% of service members wounded in action in Afghanistan and Iraq survived. According to a book by the National Academies of Sciences, Engineering, and Medicine, some of the notable medical advances during the wars include “aggressive use of tourniquets, revised transfusion principles for hemorrhagic shock, and the overall doctrine of tactical combat casualty care, defining the optimal delivery of trauma care under demanding conditions of austerity and danger.”
Medical professionals consider the higher survival rate of wounded service members in Iraq and Afghanistan all the more remarkable due to the severe and complex nature of the wounds produced by firearms, improvised explosive devices, and rocket-propelled grenades. Military medical professionals accomplished this feat in large part because of the unique specializations battlefield medicine demands. Civilian hospitals will likely not be able to produce enough medical professionals qualified to serve as flight surgeons, undersea medical specialists, or special operations medical personnel. Reductions to the military health system and outsourcing military health care to civilian hospitals threaten to disrupt adequate battlefield treatment and further advances by military medical professionals.
Conclusion
While surging funds now in order to assist with the coronavirus crisis is better than nothing, it’s backfilling a gap that should never have been created. The military’s medical capability should have always been maintained. Paring down military health facilities and laying off doctors over the past few years has reduced the military’s capacity to assist with the present health crisis and to meet the military’s future needs. It takes years to educate and train doctors, so a great deal of damage has already been done. But this can serve as a powerful lesson.
National security policy leaders should place a higher priority on the military health system and reflect that priority in the budget. There is plenty of room in the Pentagon’s budget to reallocate resources away from risky immature weapon systems to meet this need. The current proposals to shift military health care to civilian providers, which have been temporarily halted in the wake of the coronavirus pandemic, should be reevaluated once the crisis passes. Plans that make sense for normal peacetime operations are not the standard for which the military prepares itself. Any future policies must take into consideration the worst-case scenarios so we are not caught unprepared again.